The neonatal period is a unique and complex period of rapid growth and development throughout the body, thus creating unique and complex challenges in medical product development for this population. These changes may affect the safety of a product used in this population in ways that are not reflected in studies of the same product in other populations. Additionally, short term studies have not always been sufficient to identify important adverse effects in this population, as there may be latent effects that are not immediately apparent.
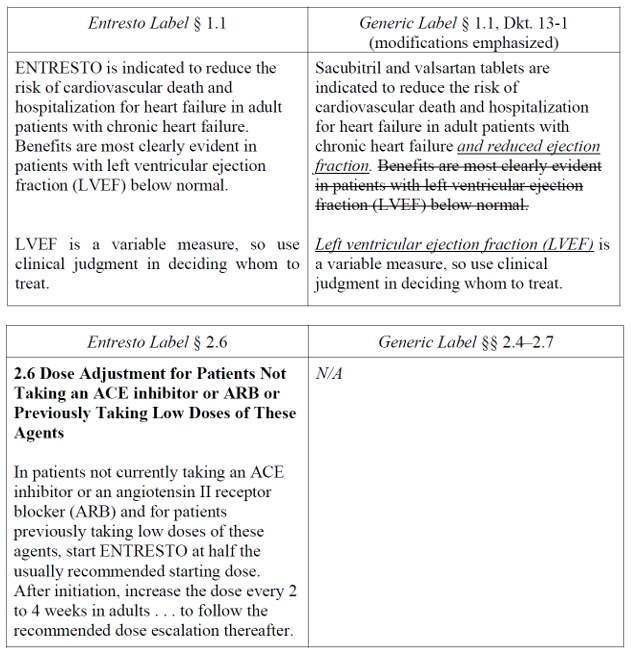
To this end, FDA recently announced the publication of a guidance titled “Considerations for Long-Term Clinical Neurodevelopmental Safety Studies in Neonatal Product Development,” (the “Guidance”). This guidance finalizes a draft guidance issued in February 2023.
For the purposes of this Guidance, the definition of “neonates” is adopted from the relevant ICH guideline as meaning day of birth plus 27 days for term and post-term infants and, for preterm infants, as meaning day of birth through expected age of delivery plus 27 days.
The Guidance is formatted to address three questions at issue:
- Is there a need for a long-term neurodevelopmental safety evaluation for neonates enrolled in clinical studies?
- What factors should be considered when developing a long-term safety study plan?
- What to measure, when, and for how long?
Is there a need for a neurodevelopmental follow-up evaluation?
To determine whether a long-term neurodevelopmental safety study is necessary, the Guidance describes general considerations, patient and population-specific considerations, and product-specific considerations that should be considered.
General considerations for this assessment include the degree of central nervous system (“CNS”) exposure; the timing of exposure relative to a particularly vulnerable stage of organ and tissue development; and the duration of exposure, as products involving repeated dosing, prolonged exposure, or with persistent effects may be associated with higher risk for long-term consequences. However, even products with single doses may require long-term safety assessments based on other considerations.
Patient and population-specific considerations include an understanding of the background rates of specific long-term neurodevelopmental outcomes in the population of interest, and disease-specific characteristics that may increase the risk for adverse neurodevelopmental outcomes.
Product-specific considerations include results from nonclinical studies conducted specifically to evaluate potential adverse effects on the developing CNS of neonates and young infants. The Guidance notes that extrapolation of data across species is challenging; however, in accord with Agency pronouncements elsewhere on this topic, the Guidance describes FDA’s limited experience with alternative assays to characterize neurodevelopmental toxicity while expressing a theoretical openness to such methods when feasible. Additional product-specific considerations include clinical pharmacology considerations, such as whether the product is thought to penetrate the CNS; clinical experience with the product in other populations; the route of administration (such as the impact of pain from repeated injections on neurodevelopment); and the nature of product components, including the active pharmaceutical ingredient, excipients, and impurities.
What factors should be considered when developing a long-term safety study plan?
If the determination is made that a long-term neurodevelopmental safety evaluation should be conducted, FDA recommends a controlled study design when feasible. Beyond that, the Guidance again describes general considerations, patient/population-specific considerations, and product-specific considerations.
General considerations include a standardization of evaluations to ensure reliability; a plan for community acceptance and inclusivity; engagement of key stakeholders to identify clinically meaningful outcomes and to assess the acceptability and feasibility of the study design; planning to keep families engaged and to maintain contact to encourage retention; and minimization of barriers to study enrollment and burdens of participation. The protocol should also include a plan for clinical referral and support services if any developmental problems are identified during the follow-up.
Patient/population-specific considerations include the timing and frequency of assessments. Neurodevelopmental safety outcomes should be evaluated up to at least 2 years of age, adjusted for prematurity. The duration and frequency of follow-up assessments depends on the nature of the outcome(s) being evaluated and the ages at which they can be reasonably measured. Sponsors should also collect relevant covariate data when other factors may influence interpretability of results in the population of interest. In most cases, a general assessment of all key neurodevelopmental domains is recommended, but if specific domains of vulnerability are known or suspected, sponsors should identify validated, age-appropriate tools to measure relevant outcomes within those domains. Additionally, the Guidance states that sponsors should provide study plans for FDA review.
Product-specific considerations include whether the product has effects on organ systems that may impact neurodevelopment and whether the product’s target changes in distribution or function throughout maturation.
What to measure, when, and for how long?
Comprehensive neurodevelopmental outcomes should be evaluated at a minimum of 2 years of age, adjusted for prematurity, though earlier and/or later evaluations of certain outcomes may also be warranted. Some evaluations can be reliably performed during the first 2 years, but others, such as subtle cognitive, language, and behavioral outcomes, may require follow-up until later in childhood even if there are no neurodevelopmental concerns observed at the initial 2-year assessment.
These evaluations should be based on well-defined and reliable clinical outcome assessments (“COAs”) that assess clearly defined concepts of interest with appropriate justification to support their use in neonatal long-term safety evaluations. Key considerations include minimizing participant burden; accounting for potential confounding factors; carefully considering the type of score to use, as some COAs may generate multiple types of scores (e.g., raw scores, standardized norm-referenced scores), some of which might present floor or ceiling effects; and ensuring that selected COAs have demonstrated reliability across demographic groups.
When a comprehensive neurodevelopmental evaluation is needed, it should include an evaluation of physical, mental, and social health. The Guidance provides a listing of domains for such assessment as pertains to general concerns (e.g., quality of life, physical health) and neurodevelopmental concerns (e.g., sensory, motor, cognition, communication).
The Guidance notes that adjunctive assessments and biomarker measures may not provide as meaningful information as long-term functional outcomes assessments and thus may not substitute for such, but they still may be useful as supportive information. This is more likely to be the case when following a known signal of concern from nonclinical studies, studies in a different population, or known effects of medical products from a similar class.
What does it all mean?
The Guidance is written carefully to communicate that these determinations are all very case-specific. It also describes all the relevant considerations as being on a sliding scale where some level of potential risk will trigger the need for and inform the design of long-term studies. Although this lack of specificity could make long-term planning challenging, we expect and hope the Agency will take an active role in answering these questions early in development.
The Guidance does not describe the proposed timing or mechanism for these studies in the context of development programs. It states that the evaluations “could be useful to support a determination of safety” for use in neonates; however, a determination of safety to support an approval is made at the time of approval.
This Guidance explicitly excludes gene therapies (a change from the draft guidance), but instead makes reference to a separate guidance that has been in place since 2020 titled Considerations for Long-Term Clinical Neurodevelopmental Safety Studies in Neonatal Product Development. In this gene therapy guidance, FDA states that: “the recommended [long-term follow-up] . . . will often not elapse for all subjects who received an investigational [gene therapy] product in the pre-marketing program before the product is licensed. Considering that, the safety data generated during clinical trials may not capture all possible delayed adverse events.” As such, FDA’s recommendations for long-term follow-up for gene therapy products include a pharmacovigilance plan in addition to the long-term follow-up study. The long-term follow-up study could be a component of the pharmacovigilance plan. It is unclear if FDA intends to treat non-gene therapy products requiring long-term follow-up similarly, but it is a reasonable assumption in the absence of information to the contrary.
FDA’s authority to require studies to support a determination of safety would be either pre-approval, as a condition for approval, or as a post-marketing requirement. Under PREA, for qualifying non-orphan designated applications, sponsors and FDA must negotiate an agreed initial pediatric study plan (iPSP) during development to be included in the application describing the sponsor’s development plans (or waiver requests) for the drug in all pediatric age groups. If the agreed iPSP is not included in the application, FDA has the authority to refuse to file (RTF) it. These requirements have generally been directed toward safety and efficacy in the relatively short term, to our knowledge. However, it seems reasonable to assume that in addition to studies typically required under PREA, sponsors will need to commit to conducting these long-term neurodevelopmental safety studies in neonates as reflected in an agreed iPSP at risk of an RTF. This highlights the importance of discussing with pediatric study plans with FDA well in advance of submitting a marketing application.
Assuming FDA intends to treat other products requiring long-term follow-up similarly to gene therapies, the long-term follow-up will not need to elapse for all subjects prior to approval. As such, the long-term follow-up would involve post-approval follow-up, perhaps in the form of a post-marketing requirement, which could be a component of pharmacovigilance. A question left unanswered is the extent of required follow-up pre-approval as a condition for approval. The answer likely is, as with most things in this Guidance, case-specific. As such, sponsors developing drugs for the neonatal population should be prepared to discuss long-term follow-up plans with FDA as early as possible to have the best understanding of regulatory requirements for approval.

{kind=link}
{kind=link}